
In engineering, “characterization” is a basic first step to understanding that which you are working with. A civil engineer may “characterize” soil and rock samples prior building a road. In my work, we perform a lot of tests to understand the behavior of laser systems. How hard can you run a diode before damage is done? How does heat, cold, humidity or vibration effect performance now and over time? You basically make changes in controlled fashion and then measure and understand all resultant moves and how they effect performance and reliability over time.
I don’t believe that I have ever seen such work (a basic characterization) done by ENT doctors to fully understand their component the “nose” and the effects of their actions on the actual performance of the “system” they are working with which is “humans”. So let’s just do that here……. In this study I set out to find easy to understand mathematical relationships that I intuitively knew existed in physics and I found them! I was tired of hearing debates regarding turbinectomies based solely on subjective non hard data results which have offered only conflicting theories for decades.
I wanted to find a way to break things down to make them as easy to understand as possible. I decided to remove all of the “mystery” I have seen in the many “limited and thus flawed” medical studies I have read by eliminating the “variability” component of each persons individual anatomy and instead learn by “characterizing” the indisputably basic round shape of a nasal turbinate in the lower half of a nasal cavity.
I already explored 3 complete models before and after surgeries and even components in isolation such as the nasal valve (here) which is a vertical slit shape. What about the cavity itself? It is a “Radial Slit”. If you look at my CT scans below, you’ll see that I “had” a perfectly normal 1..5 to 2mm “radial slit” gap of black air space which doctors then turned into a gaping 10mm hole despite no issues with this left side..

Now let’s remove all “mystery” and explore that simple radial slit shape in great detail using the scale provided above. First let’s look at the warming capacity of inspired air passing through our modeled 3cm long cavity as we expand the slit size. The table below shows vertical columns of the same size slit from top to bottom and also the (%) of distance traveled into the 3cm cavity model from 10% though the cavity to 90%. (top to bottom) 
My 5 year old girl can easily see that a thin gap quickly heats the air and a wide gap doesn’t work very well. Is this still mysterious to anyone? When I read studies that say that surgery either “doesn’t effect” or even “improves” nasal climatization I get angry. What kind of surgery? how much? measured how????? Do you see ANY step size above that produced NO change? Do you want a Turbinectomy for yourself? Your family member?
Next, lets look at other important changes. I have made this easy (trust me). For every doubling of slit size in mm you lose roughly 50% in velocity and 85% of your negative pressure (resistance). If your surgery takes you from 1mm to 4mm your pressure just dropped by 96% !!!! (You lost 85% from 1 to 2, then you lost 73% of that amount from 2 to 4 which leaves with 4% of your original pressure!!!) AND that looks just like a subtotal too doesn’t it? It also happens to closely match modeled results from my first surgery alone! (92% drop) Modeling is a VERY powerful tool and it works!
Do you want a Turbinectomy for yourself? Your family member? I didn’t think so………

In his study “Surgery of the Turbinates and Empty Nose Syndrome“, Dr. Marc Oliver Scheithauer mentions that a proper amount of shear stress is needed to trigger mucous production and cilia function. Is it any wonder ENS victims are dry? In addition to being over opened with drying air currents and turbulence they have less triggered mucous production at the same time!
“It is accepted that optimum pressure values within narrow limits in healthy people trigger both mucus production in the goblet-cells as well as the ciliary function in order to regulate mucociliary clearance on a cellular level. The precondition for this procedure is a correct balance of pressure values or shearing force on the nasal mucosa [238]. In the case of patients with ENS, these regulation mechanisms are disturbed by altered shearing forces”
So lets see where these nasal surgeries actually leave us humans (the system) in terms of having “a correct balance of pressure or shearing force” on the remaining nasal mucosa tissue. Once again I made this easy to understand. Everyone knows what it’s like to have 100 dollars and lose about 75. Terrible right? Well for every doubling of slit size, (.25 to 0.5mm, or 0.5 to 1mm, or 1mm to 2mm) you LOSE 71-74% shearing force on the walls (mucosa) as presented in “Newtons” and “Tau”.
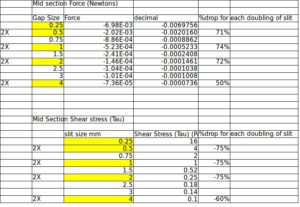
That relationship of % loss per doubling of slit fits perfectly to a power function of Force =1.0978* (slit diameter in mm)^ -1.881) The 75% loss holds until you reach 3mm, then it is a long slow roll off to infinity. Your nasal walls matter less and less.

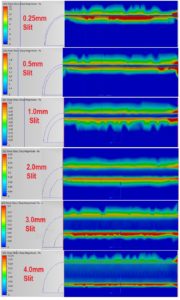
We can see these tugging forces in action below but PAY ATTENTION to the scale changes on each slit size. You will see the scale dropping like a rock following the chart above from maximums of 15 to 4 to 1.2, to 0.35, to 0.2, all the way down to 0.175. Not a lot of force to see after a subtotal turbinectomy right?
My surgeries put me at 4X past a normal 1.5-2mm gap. Do you want a Turbinectomy for yourself? Your family member? I didn’t think so………
If nerves inside the nose “were” indeed triggered by a “narrow range” of shear force, (as Dr. Marc says) then they certainly won’t function when you cut most of them out AND drastically reduce measured forces to act on any remaining nerves. Mine don’t and this is the reason ENS victims can’t sleep as my other study shows.
In the end, we must come to the sad conclusion that ENT doctors have been offering conflicting and incomplete studies regarding turbinate surgeries and their results for decades. It seems that they were they solely focused on relieving nasal obstruction and failed to understand there were any limits.
Did they even ask any questions related to ENS types of symptoms? Next, what did they actually even measure in these conflicting studies? humidification? warming capacity? resistance? particle sizes that are filtered? actual pulmonary function? sleep index for central Apneas? did they measure it before and after surgery? did they measure it 5-8 years later when ENS symptoms kick in for a some people? Did they use a large enough sample size group? did they investigate each individual type of surgery in isolation without varying the amount removed or location? Any estimated gap size recorded? Did they combine procedures by adding a septoplasty (second variable) at the same time? How long did they follow up on these test subjects? did they ask the right questions or even “fair” questions? Did they ask years later? These are all fair and scientifically reasonable questions for the kind of work they have done on humans. If they don’t have good answers then that means they have been experimenting on humans armed with only vague opinions from limited and conflicting studies. Please don’t tell me that I test my products more thoroughly doctors tested procedures intended for humans.
The point of my exercise here isn’t to try to be a coy jerk and imply that everyone needs a CFD study prior to any surgery or that every surgery needs to be an engineering project. Nor do I claim to ‘know” everything (I don’t). The point of my work here is that I have never seen anything that has assured me that ENT doctors have ever actually “quantified” much of any non subjective hard actual measurements in their studies so they do not fully understand how the nose works, when it fails, what fails or how close their interventions place you to either immediate or future damage levels.

So how large of a soft target area can comfortably exist for surgeons? Can we afford to lose 25% shear stress? 50%? half of your resistance? What do doctors actually know? What do schools teach? I fear I know the answer. My easy suggestion would be to simply look at the “normal” values that I posted here in the center area of my charts for 1.5-2mm gaps and stay close to this area. If we simply study CT scan models from “normal” people then we know what the “normal” ranges are for humans right? So then why are doctors still performing surgeries that go orders of magnitude beyond normal armed only with decades of conflicting data? Because it is easier faster and cheaper to just cut things off??? I have read most of the published CFD studies and not one of them had anything positive to say about turbinectomies yet they are still performed, even without consent. There have been a lot of detailed studies done by great doctors and researchers that have put in the work and explained most of this already, but they have just been ignored.
My lead engineer boss at work has a saying: “When (works and don’t know why) turns into (doesn’t work and don’t know why) then , you are fucked“. To be perfectly honest, if I worked like “some” ENT doctors work on noses, he would fire me in an instant.
When something fails where I work they do what is called a “Root Cause Analysis“. Every aspect of all processes, procedures, equipment and personnel is called into question and investigated. Detailed flow down charts of areas to investigate are created and sub-divide into branches of lesser degree. For example one might ask these doctors if their electrocautery devices use a standardized voltage or on time? Will doctors or their organizations pony up the money like reputable companies do to perform a proper Root Cause investigation and help repair ENS victims? At the moment, we are forced to pay for our own medical help to repair damage done by the ENT medical profession itself. If I took my car to a mechanic, and he accidentally shorted out my entire electrical system while working on it, why should I have to go to another mechanic and pay to have it fixed? That doesn’t happen in other professions because they know what they are doing. They have stated goals, specifications and measurable results.
In my line of work, when you seriously alter something you have to write a “deviation report” and file that with your product records. Years later if something fails, people can look at those records and see if that modification helped lead to failure. People with turbinectomies are ALTERED and should be given a card that says that they were “modified” like the card people get with metal joint replacements or Stapedectomy parts implanted inside one’s ear. When you have strange troubles later in life you’ll look to that card.
Last, There is a concept called a “Latent Failure”. This is where a component (like an IC chip or laser diode) is damaged but it is not detectable at that moment, however, it fails some time later after a certain amount of use and stress. I receive a LOT of messages from tortured people with screwed up noses from all over the world and some were “Latent failures”. Many ENS victims find out 5-8 years AFTER surgery that they have issues.
“I had turbinate surgery in 1991…..I have no turbinates left……Cat Scan in may 2017 confirmed this…….How do you cope? What can you tell me to prevent my suicidal ideations? I am a WiFI Engineer and I am on disability…..It seems that this didn’t really kick in until a bad sinus infection in January….I felt the paradoxal congestion ( only on the left nostril) went to 3 ENTs and they all told me I was just “dry”…..I searched the internet and found ENS , now I cannot get it out my thoughts…..Taking Klonopin at night…….life is difficult…..you seem to trudge forward…..How do you do it? ” Bruce
“I’m in search of help for my husband who has ENS for about 10 or more years!!! He’s a firemen in Houston Texas and we just figured out his problem after seeing so many doctors. Since him finding this out it has now caused him a great deal of panic and anxiety knowing what he now has. He did not have these symptoms right away. But it has gotten extremely worse over the years”! Kelly
ENT doctors fall back on their sounding board of “facts” that ENS is rare, but since they don’t measure much of anything during their studies or in actual practice of course it is rare when you don’t look. Surely some function is lost. Patients are often hard pressed to accurately describe the “feeling of obstruction” from dryness or emptiness so it is not properly attributed. ENT doctors often say that “we do this all the time and most of the time it works”. My response is this……..

B-52 Bombers in WWII were so well built that they could have parts of them shot off and still return to base. Does that mean that chopping off parts of wings is good for aviation? Do doctors attribute their “perceived” general rate of success as beneficial surgery or is it more that the human body is designed well enough to withstand a fair amount of their abuse? These doctors attend conventions every year and even after decades of “work” they are STILL debating things like this. They know there is a problem in their field yet they fail to adequately study it.

I will leave you with the remaining velocity modeling trace results from this study.
Note how the flow loses contact with the walls at 3mm and above. Do you want a Turbinectomy for yourself? Your family member? I didn’t think so………


